






Wounded Willy & Damaged Debbie
TEACHING & TRAINING PHANTOMS FOR CIVILIAN HOSPITAL EMERGENCY ROOMS
- NEW! Inclusive skin tones, from light to dark complexion, available at no additional cost
- 69 pathologies and traumas available between Willy & Debbie
- Unlimited repetition of views without human exposure
- Radiographs that permit evaluation of trainee performance
Wounded Willy & Damaged Debbie–available in realistic and inclusive skin tones–yield radiographs resembling those of a human body with human technical factors and limited artifacts, articulated to enable basic views to be presented, and with an appropriate level of human anatomy. They are well-balanced patient substitutes for basic training of radiologic technologists, particularly in military or emergency room environments.
Both Willy & Debbie demonstrate and evaluate positioning and imaging techniques, including kVp, mAs, contrast, optical density, OFD, and TFD. Their radiographs are optically equivalent to those of humans in density and contrast.
The concept of grouping a large number of casualties into two teaching/training phantoms originated at the Fleet Hospital & Operations Training Center in Camp Pendleton, California.
Product Differences
Aside from gender differences, the most obvious difference between Willy & Debbie is in the complement of traumas and pathologies assigned to each. Debbie is fitted with a wig, while Willy is bald. They are dressed in camos for military training and in jumpsuits for civilian training.
Realism of Traumas and Pathologies
“There is no single, unique description of any of their traumas and pathologies. Rather, there are limitless variations among a broad range of casualties. The most meaningful judgments of the realism of trauma and pathologies are those based on long radiographic experience across the spectrum of casualties.”
— Patrick Hale, Senior Radiologic Technologist at the UCLA Emergency Room and an RSD consultant, made those judgments with respect to Willy and Debbie.
Dimensions
At 5’ 1” (156 cm) tall, weighing 105 lbs (48 kg), Willy & Debbie match the size and weight of RSD’s Take-Apart Pixy. Technologists must learn to work with patients of all sizes and weights, so a smaller adult-size phantom is as valid for training as a larger phantom, and position is facilitated.
Lungs
Lungs are molded of durable materials with radiodensities matched to humans in a median respiratory state. Animal lungs matching the human in size and blood vessels are available, but they are oriented towards research rather than training.
Soft Tissues
Willy & Debbie have solid “soft tissues” that are hard and rigid. They cannot be palpated to locate traumas. However, radiological technologists are generally informed by the physician as to the views to be taken. The manual provides this information to instructors.
Skeletons
RSD-manufactured skeletons are used rather than natural human skeletons. The latter are generally unavailable and usually consist of an assortment of bones ranging from children to adults of ages, for which osteoporosis becomes a factor.
RSD skeletons are not to be confused with plastic skeletons for teaching anatomy. RSD skeletons are made to fit the soft-tissue molds precisely. They have spongiosa moldings within marrow cavities and outer, cortical bone. Both constituents meet the internationally accepted standards for radiodensity and specific gravity.
Neck
While anatomic fidelity and the ability to move the head into a broad range of views is required in radiography, no mechanism can be designed for intervertebral motion without artifacts obliterating the radiographs. This problem has been solved by the use of two necks. One is a multi-articulated polycarbonate assembly which provides for nearly all commonly used views. There is no attempt at radiographic realism in this neck. An alternate, fully realistic neck is interchangeable with the mechanical neck. The cervical spine of this neck contains traumas.
Model Numbers
| RS600TA | Opaque | Wounded Willy & Damaged Debbie |
| RS-600TTA | Transparent | Wounded Willy & Damaged Debbie |
| RS-601TA | Opaque | Wounded Willy |
| RS-601TTA | Transparent | Wounded Willy |
| RS-602TA | Opaque | Damaged Debbie |
| RS-602TTA | Transparent | Damaged Debbie |
Applications
- Field trauma & ER evaluation of technologist performance
- Teaching & training of patient positioning
- Image quality
- Diagnostic radiology
- Dosimetry verification
- Protocol verification
Modalities
- CT
- X-Ray
- Fluoroscopy
Anatomy
- Shoulders have ball and socket joints
- Elbows and knees flex 90° to 100°
- Broad range of positioning capabilities, including the “frog position”
- Debbie features fractures of the left shoulder and left hip plus arm and leg traumas on the right side
- Willy features traumas of both arms and legs
Clinical Images




Pathologies & Traumas (-01 to -69)
| No | Willy or Debbie | Description | Side | External Markings |
|---|---|---|---|---|
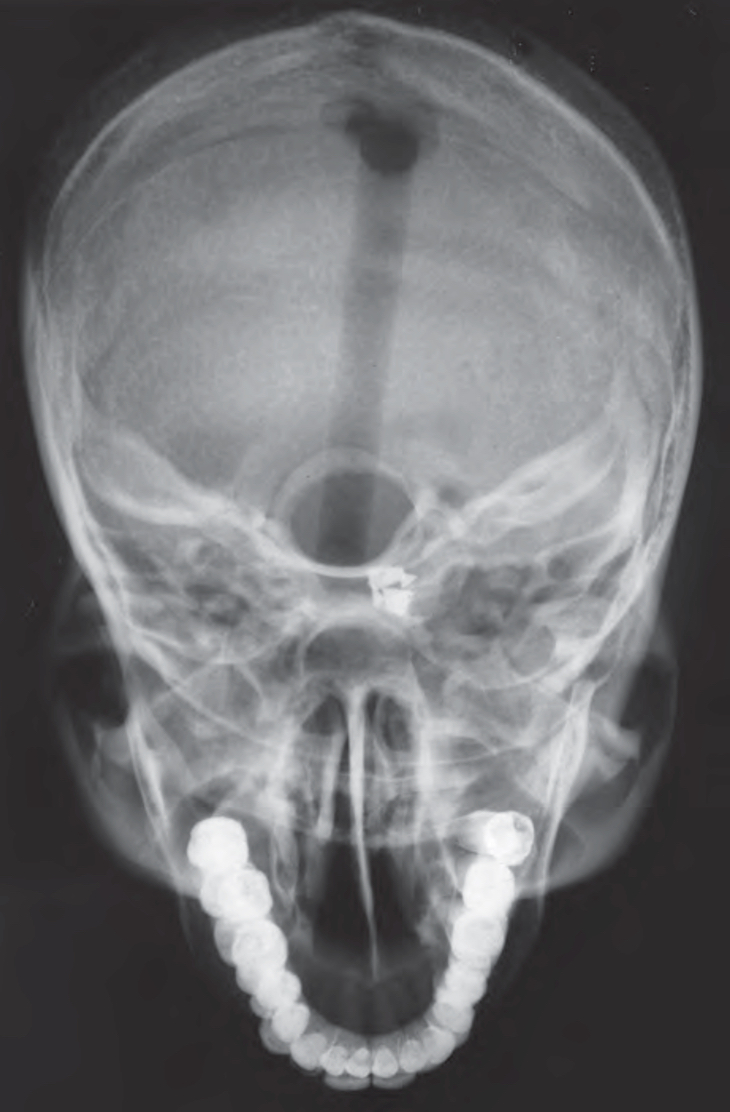
| -01 | Willy | Metallic fragment in orbit | R | None |
| -02 | Willy | Multiple fragments in lower face | N/A | None |
| -03 | Willy | Step deformity of intraorbital rim | L | None |
| -04 | Willy | Separated fracture of frontal zygomatic suture | L | None |
| -05 | Willy | Metallic foreign body over skull | N/A | None |
| -06 | Willy | Mandible fracture with missing bone | N/A | Open wound |
| -07 | Debbie | Mandibular fractures | R | None |
| -08 | Debbie | Mandibular fractures | L | None |
| -09 | Debbie | Cloudy maxillary sinus | L | None |
| -10 | Debbie | Fracture of nasal bones with mild displacement | N/A | None |
| -11 | Willy | Displacement fracture of mandibular condyle & coronoid process | R | None |
| -12 | Willy | Displacement fracture of mandibular condyle & coronoid process | L | None |
| -13 | Willy | C4/C5 compression fracture | N/A | None |
| -14 | Willy | C7 fractured by bullet | R | Bullet or foreign body hole |
| -15 | Willy | C-spine bullet posterior to trachea shadow | N/A | Bullet or foreign body hole |
| -16 | Willy | Fracture of lateral ribs 6 & 7 | R | None |
| -17 | Willy | Mediolateral fracture of ribs 8 & 9 | L | None |
| -18 | Willy | Multiple rib fractures, four metallic fragments visible | R | None |
| -19 | Willy | 12th rib fracture | R | None |
| -20 | Willy | Bullet in hemothorax overlaying 8th rib | L | Bullet or foreign body hole |
| -21 | Willy | Bullet in mid-chest overlaying heart shadow | L | None |
| -22 | Willy | 2cm metallic fragment mid-chest | R | Bullet or foreign body hole |
| -23 | Willy | Bullet visible below costal margin under 11th rib | L | Bullet or foreign body hole |
| -24 | Willy | One bullet in lower quadrant | R | Bullet or foreign body hole |
| -25 | Willy | Shattered distal scapulae, three metallic fragments | R | Bullet or foreign body hole |
| -26 | Willy | Shattered distal scapulae | L | Bullet or foreign body hole |
| -27 | Debbie | Widened mediastinum & pleural effusion | L | None |
| -28 | Debbie | Chest tube cavity | R | Bullet or foreign body hole |
| -29 | Debbie | Infiltrate | R | None |
| -30 | Debbie | Infiltrate | L | None |
| -31 | Debbie | Bullet in mid-chest | N/A | Bullet or foreign body hole |
| -32 | Willy | Unstable fracture of L1 | N/A | None |
| -33 | Willy | Compression fracture of L5 | N/A | None |
| -34 | Debbie | Metallic foreign body lateral to PSOAS | R | Bullet or foreign body hole |
| -35 | Debbie | Compression fracture of L4 | N/A | None |
| -36 | Debbie | Metallic fragments, mid-abdomen in LQ | L | Bullet or foreign body hole |
| -37 | Debbie | Bullet in mid-abdomen in RQ | R | Bullet or foreign body hole |
| -38 | Debbie | Metallic fragments, three in RUQ back | R | Bullet or foreign body hole |
| -39 | Debbie | Metallic fragments, two in LUQ back | L | Bullet or foreign body hole |
| -40 | Willy | ILIAC crest comminuted fracture with metallic fragments in left quadrant | L | Bruise |
| -41 | Debbie | Displaced fracture of pubic ramus, superior & inferior | L | None |
| -42 | Debbie | Sacroiliac disruption | L | None |
| -43 | Debbie | Fractured sternum | N/A | None |
| -44 | Willy | Non-displaced pubic ramus fracture | L | None |
| -45 | Willy | Superior & inferior pubic ramus fracture | R | None |
| -46 | Willy | Symphysis diastasis | N/A | None |
| -47 | Willy | Sacroiliac joint disruption | R | None |
| -48 | Willy | Bullet in sacrum | R | None |
| -49 | Willy | Shattered acetabulum | L | None |
| -50 | Willy | Shattered femoral head | L | None |
| -51 | Willy | Left femur comminuted fracture | L | None |
| -52 | Debbie | Proximal tibia fracture | L | None |
| -53 | Willy | Comminuted fracture of tibia and fibula | R | Bullet or foreign body hole |
| -54 | Willy | Displaced ankle fracture | R | None |
| -55 | Debbie | Minimally displaced distal fibula fracture | R | None |
| -56 | Debbie | Displaced fracture of calcaneus bone | R | None |
| -57 | Willy | Displaced fracture of radius and ulna | L | None |
| -58 | Debbie | Volar angulated distal radius and ulna fracture | R | Bullet or foreign body hole |
| -59 | Willy | Angulated comminuted fracture of mid-shaft radius and ulna | R | None |
| -60 | Debbie | Minimally displaced distal radius fracture not involving wrist, offset bone ends | L | None |
| -61 | Debbie | Humerus shaft fracture | L | None |
| -62 | Debbie | Femur fracture | L | None |
| -63 | Debbie | Scapulae shattered with two metal fragments on right | R | None |
| -64 | Debbie | Scapulae shattered with one metal fragments on left | L | None |
| -65 | Willy | Two metallic fragments on right superior angle | R | None |
| -66 | Willy | Three metallic fragments on left superior angle | L | None |
| -67 | Willy | 3rd and 4th meracarpals shattered | L | Bruised |
| -68 | Willy | Glenoid fracture on left scapular | L | None |
| -69 | Debbie | Radius fracture | L | None |